What substances are characterized by an active reabsorption mechanism? Tubular reabsorption and its regulation
The human excretory system enters the human body and removes metabolic products. The work of the organs of the human excretory system has its own mechanisms for removing metabolic products, formed in the process of evolution, which are filtration, reabsorption and secretion.
Human excretory system
The elimination of metabolic products from the body is carried out by the kidneys, ureters, bladder and urethra.
The kidneys are located in the retroperitoneal space in the area lumbar region and are bean-shaped.
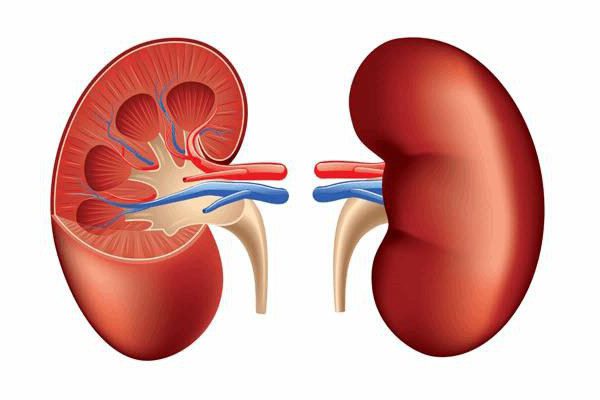
This is a paired organ consisting of the cortex and medulla, the pelvis, and it is covered with a fibrous membrane. The renal pelvis consists of a small and large cup, and from it comes the ureter, which delivers urine to the bladder and through the urethra the final urine is removed from the body.
The kidneys are involved in metabolic processes, and their role is in ensuring the body’s water balance, maintaining acid-base balance are fundamental to the full existence of a person.
The structure of the kidney is very complex and its structural element is the nephron.

It has a complex structure and consists of a proximal canal, a nephron corpuscle, a loop of Henle, a distal canal and a collecting duct that gives rise to the ureters. Reabsorption in the kidneys occurs through the proximal and distal tubules and the loop of Henle.
Reabsorption mechanism
The molecular mechanisms of the passage of substances during the reabsorption process are:
- diffusion;
- endocytosis;
- pinocytosis;
- passive transport;
- active transport.
Of particular importance for reabsorption are active and passive transport and the direction of reabsorbed substances along the electrochemical gradient and the presence of a carrier for substances, the operation of cellular pumps and other characteristics.

The substance goes against the electrochemical gradient with the expenditure of energy for its implementation and through special transport systems. The nature of the movement is transcellular, which is carried out by passing through the apical and basolateral membranes. Such systems are:
- Primary active transport, which is carried out using energy from the breakdown of ATP. It is used by Na+, Ca+, K+, H+ ions.
- Secondary active transport occurs due to the difference in the concentration of sodium ions in the cytoplasm and in the lumen of the tubules, and this difference is explained by the release of sodium ions into the intercellular fluid with the expenditure of energy from the breakdown of ATP. It is used by amino acids and glucose.
It passes along gradients: electrochemical, osmotic, concentration, and its implementation does not require energy expenditure or the formation of a carrier. The substances that use it are Cl- ions. The movement of substances is paracellular. This is movement through the cell membrane, which is located between two cells. Characteristic molecular mechanisms are diffusion and solvent transport.
The process of protein reabsorption takes place inside the cellular fluid, and, after breaking it down into amino acids, they enter the intercellular fluid, which occurs as a result of pinocytosis.
Types of reabsorption
Reabsorption is a process that takes place in the tubules. And substances passing through the tubules have different transporters and mechanisms.

Per day, from 150 to 170 liters of primary urine are formed in the kidneys, which undergoes a process of reabsorption and returns to the body. Substances with highly dispersed components cannot pass through the tubular membrane and, during the process of reabsorption, enter the blood with other substances.
Proximal reabsorption
In the proximal nephron, which is located in the renal cortex, reabsorption takes place for glucose, sodium, water, amino acids, vitamins and protein.

The proximal tubule is formed by epithelial cells that have an apical membrane and a brush border, and it faces the lumen of the renal tubules. The basement membrane forms folds that form the basal labyrinth, and through them primary urine enters the peritubular capillaries. The cells are tightly connected to each other and form a space that runs throughout the intercellular space of the tubule, and it is called the basolateral labyrinth.
Sodium reabsorption has a complex three-step process, and it is a carrier for other substances.
Reabsorption of ions, glucose and amino acids in the proximal tubule
The main stages of sodium reabsorption:
- Passage through the apical membrane. This is the stage of passive sodium transport, through Na channels and Na transporters. Sodium ions enter the cell through membrane hydrophilic proteins that form Na channels.
- The entry or passage through the membrane is associated with the exchange of Na+ for hydrogen, for example, or with its entry as a carrier of glucose or amino acid.
- Passage through the basement membrane. This is the stage of active transport of Na+, through Na+/K+ pumps with the help of the enzyme ATP, which releases energy when broken down. Sodium, being reabsorbed in the renal tubules, constantly returns to metabolic processes and its concentration in the cells of the proximal tubule is low.
Reabsorption of glucose occurs through secondary active transport and its intake is facilitated by its transfer through the Na pump, and it is completely returned to metabolic processes in the body. The increased concentration of glucose is not completely reabsorbed in the kidneys and is excreted in the final urine.

Reabsorption of amino acids occurs similarly to glucose, but the complex organization of amino acids requires the participation of special transporters for each amino acid with less than 5-7 additional ones.
Reabsorption in the loop of Henle
The loop of Henle passes through and the reabsorption process in the ascending and descending parts of it is different for water and ions.
The filtrate, entering the downward part of the loop and going down it, releases water due to a different pressure gradient and is saturated with sodium and chlorine ions. In this part, water is reabsorbed, and it is impermeable to ions. The ascending part is impermeable to water and when passing through it, the primary urine is diluted, while in the descending part it is concentrated.
Distal reabsorption
This section of the nephron is located in the renal cortex. Its function is to reabsorb water, which is collected in primary urine and exposes sodium ions to reabsorption. Distal reabsorption is the dilution of primary urine and the formation of final urine from the filtrate.
Entering the distal tubule, primary urine in a volume of 15% after reabsorption in the renal tubules makes up 1% of the total volume. After collecting in the collecting duct, it is diluted and the final urine is formed.
Neurohumoral regulation of reabsorption
Reabsorption in the kidneys is regulated by the sympathetic nervous system and thyroid hormones, hypothalamic-pituitary and androgens.
Reabsorption of sodium, water, and glucose increases when the sympathetic and vagus nerves are excited.
The distal tubules and collecting ducts reabsorb water in the kidneys under the influence of antidiuretic hormone or vasopressin, which increases when water in the body decreases. large quantities, and the permeability of the tubule walls also increases.
Aldosterone increases the reabsorption of calcium, chloride and water, as does atriopeptide, which is produced in the right atrium. Suppression of sodium reabsorption in the proximal nephron occurs when parathyrin enters.
Activation of sodium reabsorption occurs due to hormones:
- Vasopressin.
- Glucogan.
- Calcitonin.
- Aldosterone.
Inhibition of sodium reabsorption occurs during the production of hormones:
- Prostaglandin and prostaglandin E.
- Atriopeptide.
The cerebral cortex regulates the excretion or inhibition of urine.
Tubular reabsorption of water is carried out by a variety of hormones responsible for the permeability of the membranes of the distal nephron, the regulation of its transport along the tubules, and much more.
Reabsorption value
The practical application of scientific knowledge about what reabsorption is in medicine has made it possible to obtain information confirmation about the work of the body’s excretory system and to look into its internal mechanisms. goes through very complex mechanisms and influences on it environment, genetic abnormalities. And they do not go unnoticed when problems arise against their background. In a word, health is very important. Keep an eye on it and all the processes occurring in the body.
The main function of the kidneys is to process and remove toxic substances and harmful compounds from the body. During normal operation of this organ, a person has standard blood pressure, the formation of the hormone erythropoietin occurs, and balanced homeostasis is achieved. The process of urine formation occurs in three important stages: filtration, reabsorption and secretion. Reabsorption is the absorption of components of different origins from the urinary fluid.
Reabsorption of substances occurs through the renal channels, with the participation of epithelial cells. The latter perform the function of an absorbent; it is in them that the elements are distributed and they contain filtration products. The process of absorption of glucose, water, amino acids, sodium, and various ions is also carried out, they are transported directly into the circulatory system.
Chemical substances that are a consequence of the breakdown of products are contained in large quantities in the body, and these cells filter them out. Absorption occurs in the proximal canals. After this, the filtering mechanism chemical elements moves into the loop of Henle, collecting ducts and distal convoluted tubules. The reabsorption stage is characterized by maximum absorption of ions necessary for the proper functioning of the body and chemical substances. There are several routes of absorption organic compounds:
- Active. The movement of substances is carried out against an electrochemical, concentrated gradient: sodium, magnesium, glucose, amino acids and potassium.
- Passive. It is distinguished by the transfer of necessary substances along an osmotic, concentration, electrochemical gradient: urea, water, bicarbonates.
- Movement by pinocytosis: protein.
Reabsorption processes in the kidney tubules
The level and speed of cleaning, moving the necessary elements and connections depends on various factors. Primarily from food, lifestyle, and the presence of chronic diseases. Each of these aspects affects the functioning of the entire body, because if the kidneys are malfunctioning, all systems suffer.
There are several types of reabsorption, each of them depends on the area of the tubules in which the distribution of useful components occurs. There are two types of reabsorption:
- distal;
- proximal.
The latter is distinguished by the ability of these channels to transport and secrete protein, amino acids, water, vitamins, chlorine, sodium, vitamins, dextrose and trace elements from primary type urine. There are several aspects to this process:
- Water is released through a passive movement mechanism. The quality and speed of this process largely depends on the presence of alkali and hydrochloride in the purification products.
- Bicarbonate is transported through the implementation of a passive and active mechanism. The intensity of absorption largely depends on the part of the organ through which primary urine moves. Passage through the tubules occurs in a dynamic mode. Absorption through the membrane requires some time. Passive transportation is characterized by a decrease in urine volume, as well as an increase in bicarbonate concentration.
- The movement of dextrose and amino acids is carried out by epithelial tissue. These elements are localized in the alkaline zone of the apical membrane. These components are absorbed, and hydrochloride is simultaneously formed. The process is characterized by a decrease in bicarbonate concentration.
- When glucose is released, maximum connection with the moving cells occurs. If the glucose concentration is significant, then the load on transport cells increases. This process leads to the fact that glucose does not pass into the blood supply.

Processes occurring in the proximal tubule
(yellow indicates active Na+,K+ transport)
The proximal mechanism is characterized by maximum protein and peptide uptake. In this case, the absorption of substances occurs in full force. Refining accounts for only 30% of the total nutrients. The distal variety changes the final composition of urine and also affects the concentration of organic compounds. At this stage, alkali is absorbed and the passive type of calcium, potassium, chloride and phosphates are transferred.
If the process of inadequate filtration occurs or dysfunction of the cleansing organs occurs, then there is a high probability of all sorts of pathologies and problems occurring. All of them have characteristic symptoms and require immediate treatment, otherwise serious complications can occur. Such problems include the following aspects:
- Impaired tubular reabsorption. A decrease or increase in absorption capacity, which manifests itself in a lack of water, ions and organic compounds directly from the lumens of the tubules. Dysfunction appears due to reduced activity of transporting substances, lack of macroergs and transporters, as well as damage to the epithelial layer.
- Renal syndromes are a consequence of a disruption in the rhythm of urination, diuresis, changes in the color of urine and its composition. These syndromes cause renal failure and tubulopathy.
- Problems with the secretion of epithelial cells. Damage to the distal parts of the canals, mechanical impact on the medulla/cortical layers or kidney tissue. In the presence of dysfunction, the likelihood of extrarenal and renal symptoms is high.
- Oliguria – the volume of daily urine decreases, while the specific gravity of urine increases.
- Polyuria is diuresis, the specific gravity of the fluid decreases.
- Hormonal imbalance. This result is caused by the intensive production of aldosterone, which results in increased sodium absorption, which provokes a large accumulation of fluid in the body, due to which the amount of potassium decreases and increased swelling of some parts of the body appears.
- Problems with the structure of the epithelium. This pathology is the main factor provoking a lack of control over urine concentration.

Oliguria is a condition in which urine production in the body is reduced.
The exact cause of the negative state of the body is determined through laboratory urine analysis. That is why, in case of any deterioration in your health, you should contact a medical facility. After a series of diagnostic measures, the exact cause of the pathology can be determined. Based on the data obtained, the most appropriate, rational and affordable treatment plan is drawn up.
To accurately determine the mechanism of proximal reabsorption, it is necessary to determine the level of glucose concentration in the body, focusing on the highest indicator. Laboratory assessment has a number of very important aspects that you should pay attention to:
- The rate of glucose reabsorption is determined by administering a sugar solution intravenously to the patient; this mixture significantly increases the level of glucose in the circulatory system.
- After this, a urine test is performed. If the content is in the range of 9.5-10 mmol per liter, then it is considered normal.
- Determining distal reabsorption is no less important, although this process also has several features:
- For a certain period of time, the patient should refrain from drinking any liquid.
- Urine is taken for analysis, and the condition of the fluid itself, as well as its plasma, is examined.
- After a certain period of time, the patient is administered vasopressin.
- Then you can drink water.

The patient should refrain from drinking any liquid for a certain period of time.
After receiving data on the body’s reaction, the presence of nephrogenic or insipidus diabetes can be recorded.
During normal functioning of the urinary system, toxic compounds and food breakdown products are systematically and timely removed from the body. If the first signs of kidney dysfunction appear, then you cannot proceed to independent treatment, but you need to contact an experienced specialist. If treatment is not started on time, then there is a high probability of various complications occurring, as well as some diseases becoming chronic.
Process regulation
Blood circulation of the kidneys is a relatively autonomous process. If change blood pressure carried out from 90 mm to 190 mm. rt. Art., then the pressure in the renal capillaries is maintained at a normal level. This stability can be explained by the fact that there is a certain difference in diameter between the efferent and influent vessels of the circulatory system. Regulation is a very important aspect in the operation of this system; there are two main methods: humoral and myogenic autoregulation.
Myogenic, with an increase in blood pressure in the afferent alveoli, contracts, as a result of which less blood flows into the organ, due to which the pressure stabilizes. As a rule, contraction is provoked by angiotensin II; leukotrienes and thromboxanes have the same principle of action. Substances that dilate blood vessels are dopamine, acetylcholine and others. Due to their influence, the pressure in the glomerular capillaries is normalized, which makes it possible to maintain a normal GFR value.
Humoral is realized through hormones. The main characteristic of tubular reabsorption is the rate of water absorption. This process can be safely divided into two stages: mandatory, in which all manipulations occur in the proximal tubules, there is no dependence on the water load, and dependent, it is carried out in the collecting ducts and distal tubules. Vasopressin is considered the main hormone in this process; it promotes water retention in the body. This compound is synthesized by the hypothalamus, after which it is transported to the neurohypophysis and then to the circulatory system.
Tubular reabsorption is a mechanism that organizes the process of returning nutrients, trace elements and water to the blood. Reabsorption occurs on all parts of the nephron, although different patterns occur. Violation of this process leads to serious complications and consequences. That is why, if you have the first signs of problems, you should contact a medical institution and undergo an examination, otherwise there is a possibility.
The role of the kidneys in human body invaluable. These vital organs perform many functions, they regulate blood volume, eliminate waste products from the body, normalize acid-base and water-salt balance, etc. These processes are carried out due to the fact that urine formation occurs in the body. Tubular reabsorption refers to one of the stages of this important process, which affects the activity of the entire organism as a whole.
The importance of the body's excretory system
Removing the end products of tissue metabolism from the body is a very important process, since these products are no longer capable of bringing benefit, but can have a toxic effect on humans.
Excretory organs include:
- leather;
- intestines;
- kidneys;
- lungs.
The formation of atrial natriuretic hormone occurs in the atria when they are stretched due to excess blood. This hormonal substance, on the contrary, reduces the absorption of water in the distal tubules, enhancing the process of urine formation and facilitating the removal of excess fluid from the body.
What violations can there be?
Kidney diseases can be caused by various reasons, among which pathological changes in reabsorption are not last place. In case of impaired absorption of water, a pathological increase may develop, as well as in which it is less than one liter.
Impaired absorption of glucose leads to a condition in which this substance is not reabsorbed at all and is completely excreted from the body along with urine.
Very dangerous acute condition renal failure, when kidney function is impaired and organs stop functioning normally.
Details
Reabsorption is the transport of substances from the lumen of the renal tubules into the blood flowing through the peritubular capillaries. Reabsorbed 65% of the volume of primary urine(approximately 120 l/day. It was 170 l, 1.5 was released): water, mineral salts, all necessary organic components (glucose, amino acids). Transport passive(osmosis, diffusion along an electrochemical gradient) and active(primary active and secondary active with the participation of protein carrier molecules). Transport systems are the same as in the small intestine.
Threshold substances - usually completely reabsorbed(glucose, amino acids) and are excreted in the urine only if their concentration in the blood plasma exceeds a threshold value (the so-called “excretion threshold”). For glucose, the elimination threshold is 10 mmol/l (with a normal blood glucose concentration of 4.4-6.6 mmol/l).
Non-threshold substances are always excreted regardless of their concentration in the blood plasma. They are not reabsorbed or are partially reabsorbed, for example, urea and other metabolites.
The mechanism of operation of various parts of the renal filter.
1. In the proximal tubule the process of concentrating the glomerular filtrate begins, and the most important point here is the active absorption of salts. With the help of active transport, about 67% of Na+ is reabsorbed from this section of the tubule. An almost proportionate amount of water and some other solutes, such as chloride ions, follow the sodium ions passively. Thus, before the filtrate reaches the loop of Henle, about 75% of the substances from it will be reabsorbed. As a result, the tubular fluid becomes isosmotic with respect to blood plasma and tissue fluids.
The proximal tubule is ideally suited for intensive reabsorption of salt and water. Numerous microvilli of the epithelium form the so-called brush border, covering the inner surface of the lumen of the renal tubule. With this arrangement of the absorbent surface, the area of the cell membrane increases enormously and, as a result, the diffusion of salt and water from the lumen of the tubule into the epithelial cells is facilitated.
2. Descending limb of the loop of Henle and part of the ascending limb, located in the inner layer medulla, consist of very thin cells that do not have a brush border, and the number of mitochondria is small. The morphology of thin sections of the nephron indicates the absence of active transport of solutes through the wall of the tubule. In this area of the nephron, NaCl penetrates very poorly through the wall of the tubule, urea - somewhat better, and water passes through without difficulty.
3. Wall of the thin portion of the ascending limb of the loop of Henle also inactive regarding salt transport. However, it is highly permeable to Na+ and Cl-, but low permeable to urea and almost impermeable to water.
4. Thick portion of the ascending limb of the loop of Henle, located in the renal medulla, differs from the rest of the said loop. It actively transports Na+ and Cl- from the lumen of the loop into the interstitial space. This section of the nephron, together with the rest of the ascending limb, is extremely little permeable to water. Due to NaCl reabsorption, fluid enters the distal tubule somewhat hypoosmotic compared to tissue fluid
5. Movement of water through the wall of the distal tubule- the process is complex. The distal tubule is of particular importance for the transport of K+, H+ and NH3 from the tissue fluid into the nephron lumen and the transport of Na+, Cl- and H2O from the nephron lumen into the tissue fluid. Since salts are actively “pumped out” from the lumen of the tubule, water follows them passively.
6. Collecting duct permeable to water, allowing it to pass from dilute urine into the more concentrated tissue fluid of the renal medulla. This is the final stage of the formation of hyperosmotic urine. Reabsorption of NaCl also occurs in the duct, but due to the active transfer of Na+ through the wall. The collecting duct is impermeable to salts, but its permeability varies with respect to water. Important feature The distal portion of the collecting duct, located in the inner medulla of the kidneys, is its high permeability to urea.

Mechanism of glucose reabsorption.
Proximal(1/3) glucose reabsorption is carried out using special transporters of the brush border of the apical membrane of epithelial cells. These transporters transport glucose only if they simultaneously bind and transport sodium. Passive movement of sodium along the concentration gradient into cells leads to transport across the membrane and transporter with glucose.
To implement this process, a low concentration of sodium in the epithelial cell is required, creating a concentration gradient between the external and intracellular environment, which is ensured by energy-dependent work basement membrane sodium-potassium pump.
This type of transport is called secondary active, or simport, i.e., joint passive transport of one substance (glucose) due to the active transport of another (sodium) using one carrier. If there is an excess of glucose in the primary urine, all transport molecules may be completely loaded and glucose will no longer be able to be absorbed into the blood.
This situation is characterized by the concept “ maximum tubular transport of substance"(Tm glucose), which reflects the maximum load of tubular transporters at a certain concentration of the substance in the primary urine and, accordingly, in the blood. This value ranges from 303 mg/min in women to 375 mg/min in men. The value of maximum tubular transport corresponds to the concept of “renal excretion threshold”.
Renal excretion threshold they call that one concentration of a substance in the blood and, accordingly, in primary urine, in which it can no longer be completely reabsorbed in the tubules and appears in the final urine. Such substances for which an excretion threshold can be found, i.e., completely reabsorbed at low concentrations in the blood, but not completely at elevated concentrations, are called threshold substances. An example is glucose, which is completely absorbed from the primary urine at plasma concentrations below 10 mmol/L, but appears in the final urine, i.e., is not completely reabsorbed, when its content in the blood plasma is above 10 mmol/L. Hence, for glucose, the elimination threshold is 10 mmol/l.

Secretion mechanisms in the renal filter.
Secretion is the transport of substances from the blood flowing through the peritubular capillaries into the lumen of the renal tubules. Transport is passive and active. H+, K+ ions, ammonia, organic acids and bases are secreted (for example, foreign substances, in particular drugs: penicillin, etc.). Secretion of organic acids and bases occurs via a secondary active sodium-dependent mechanism.

Secretion of potassium ions.
Most of the potassium ions easily filtered in the glomeruli are usually reabsorbed from the filtrate in the proximal tubules and loops of Henle. The rate of active reabsorption in the tubule and loop does not decrease even when the concentration of K+ in the blood and filtrate increases greatly in response to the body's excess consumption of this ion.
However, the distal tubules and collecting ducts are capable of not only reabsorbing, but also secreting potassium ions. By secreting potassium, these structures strive to achieve ionic homeostasis if they enter the body in an unusually large quantity this metal. Transport of K+ appears to depend on its entry into tubular cells from the tissue fluid, due to the activity of the usual Nar+ - Ka+ pump, with leakage of K+ from the cytoplasm into the tubular fluid. Potassium can simply diffuse along an electrochemical gradient from the renal tubular cells into the lumen because the tubular fluid is electronegative with respect to the cytoplasm. K+ secretion through these mechanisms is stimulated by the adrenocortical hormone aldosterone, which is released in response to an increase in K+ levels in the blood plasma.
The kidneys, depending on the body’s water balance, can secrete both diluted and concentrated urine. All parts of the tubules and the renal medulla participate in this process. About 1% of the fluid filtered in the glomeruli is excreted in the urine, and 99% is reabsorbed in the tubules. Water reabsorption is a passive process and is carried out using osmotic pressure along a concentration gradient.
The movement of water depends mainly on the transport of sodium ions. Removal of sodium from the tubule occurs with the expenditure of energy, i.e. actively, water follows sodium passively as a result of the resulting difference in osmotic pressure on either side of the tubular cells. Sodium and water are removed at the same rate.
In the proximal convoluted tubule, 80-85% of the total amount of glomerular filtrate is reabsorbed. The rate of reabsorption here is constant and practically does not depend on the antidiuretic hormone. Such reabsorption is called obligate (from Latin obligatio - obligatory). The remaining 15-20% of the glomerular filtrate is reabsorbed in the distal nephron and depends on the action of ADH. Such reabsorption is called facultative (from Latin facultas - opportunity, opportunity). With excessive water consumption, the amount of urine, diuresis, increases and can amount to up to 15% of the glomerular filtrate. This is called water diuresis. On the contrary, with loss of water and dehydration of the body, the water in the tubules is almost completely reabsorbed, urine is not excreted - antidiuresis occurs.
This regulation of water secretion occurs in the distal nephron under action of ADH. Dehydration and an increase in plasma electrolytes (increase in osmolality) stimulates the secretion of ADH; excess water and decreased osmolality reduce the secretion of antidiuretic hormone.
The constancy of the volume of blood and extracellular fluid and the stability of osmotic pressure are in the body under the control of the central nervous system(CNS) with the help of sensitive receptors, osmoreceptors, located in various organs and tissues. From the receptors, information about changes in osmotic pressure is transmitted to the hypothalamus, this is a stimulus for the secretion of antidiuretic hormone. An important stimulus for ADH secretion is the volume of circulating blood. An increase in blood flow to the heart with an increase in circulating blood volume is accompanied by a decrease in ADH secretion, while the excretion of water and sodium in the urine increases and the original blood volume is restored.
The secretion of antidiuretic hormone depends on emotions such as pain, anxiety, nervous tension, as well as on the administration of certain medications and other factors. A pathological decrease in ADH secretion leads to a significant increase in water excretion by the kidneys, which is observed in patients with diabetes insipidus. Treatment is with vasopressin.